Part 1
Disclaimer: I am not a medical professional. The content of these blog posts is based on my own experience, research, and conversations with my doctors – and my subsequent questions. Always talk to your doctor before making any changes to your medications, diet, or activity. There’s also a lot of conjecture and curiosity in these posts, with as many questions as there are answers on this evolving topic.
In last week’s post, we explored the body’s Endocannabinoid System and how protecting it is vital for health and stress management. [1] Supplementing with plant-based cannabinoids appears to have benefits when sleep, exercise, and proper diet aren’t enough, but I also wanted to understand the potential drawbacks of using cannabis for stress management, which is taking me down an Alice in Wonderland-type rabbit hole of research, resulting in more questions than answers, from brain chemistry to metaphysics.
As I’ve mentioned in recent posts, protecting my brain is a priority for me. When one of my doctors recommended medical marijuana (and another advised against it, only because “it’s expensive”), I really wanted a better understanding of the benefits and drawbacks. There are clearly demonstrated health benefits associated with better sleep and lower stress levels, which could be achieved with certain cannabis products. I would love to improve my ability to think more clearly, prioritize work more effectively, and strategize better with a clear and well-rested head.
Image credit: [2]
That said, I do have concerns about whether my language skills would be impacted in the long term and whether I have any IQ points to spare at this age: I rely on my brain for my living and need to quickly and clearly convey thoughts (and rebuttals) regarding contentious relevant issues. And unfortunately, there’s a lot we still don’t know about the long-term impacts of cannabis on the human body because it has been so heavily restricted for more than 50 years, which has even limited our ability to study its benefits (not just its harms).
Schedule I
After a variety of steps to restrict and criminalize the use of marijuana as early as 1937, the Controlled Substances Act of 1970 officially made it federally illegal. In 1972 it was categorized as a Schedule I drug, indicating that it has no medicinal benefits and a high likelihood for abuse, despite regular evidence to the contrary on both counts. It has been documented at this point that the Nixon administration’s push to schedule marijuana in the most dangerous category of drugs was for political reasons, in hopes of silencing many among the anti-war left. (There was also a history of racism informing that and earlier policies.) [3]
For reference, other Schedule I drugs include heroin and ecstasy (MDMA); Schedule II drugs (which have some medical uses but also high potential for addiction) include oxycodone and fentanyl; Schedule III drugs include ketamine and acetaminophen with codeine; Schedule IV, Xanax and Ambien; and Schedule V (accepted medical use and low potential for abuse), Robitussin and Lyrica. [4] Despite the current limitations around studying cannabis, many in the medical community have openly recognized its medicinal benefits in recent years, regularly calling for rescheduling.
Image credit: [5]
Several recent presidents have spoken about the possibility of rescheduling cannabis, but that has yet to happen. [6],[7] Meanwhile, multiple states have legalized it recreationally or medically, but even a medical need doesn’t help anyone with a federal job that prohibits cannabis use, and state laws don’t help the state of research. As I try to evaluate my options, it’s clear that I still don’t have sufficient information to make an informed decision because research has been difficult to conduct for more than 50 years.
Educated Guesses
At this point, I have more questions than answers, but some of my preliminary research uncovered interesting and unexpected findings. Despite years’ worth of warnings during D.A.R.E. Program [8] classes when I was a kid, to the best of our knowledge, the jury appears to be out on whether cannabis actually kills brain cells. Heavy, long-term marijuana use is correlated with short- and long-term impacts to brain function, [9] but what we define as “brain function” can vary. A 25-year study of young adults found that long-term marijuana use was associated with impaired verbal memory but that there was no evidence of harm to cognitive processing or executive function. [10]
Even studies of teenagers (where we know there is more potential for harm) are split, with one showing lower IQs for those who used marijuana during adolescence and one showing no difference in gray matter use on MRI scans. [11] One study of note compared the negative impacts of alcohol vs. cannabis, and the risks to brain health were far clearer with the former [12] – and we’ve had legal alcohol use for adults since 1933, despite clear evidence of health harms. (That sounds like fodder for a blog post!)
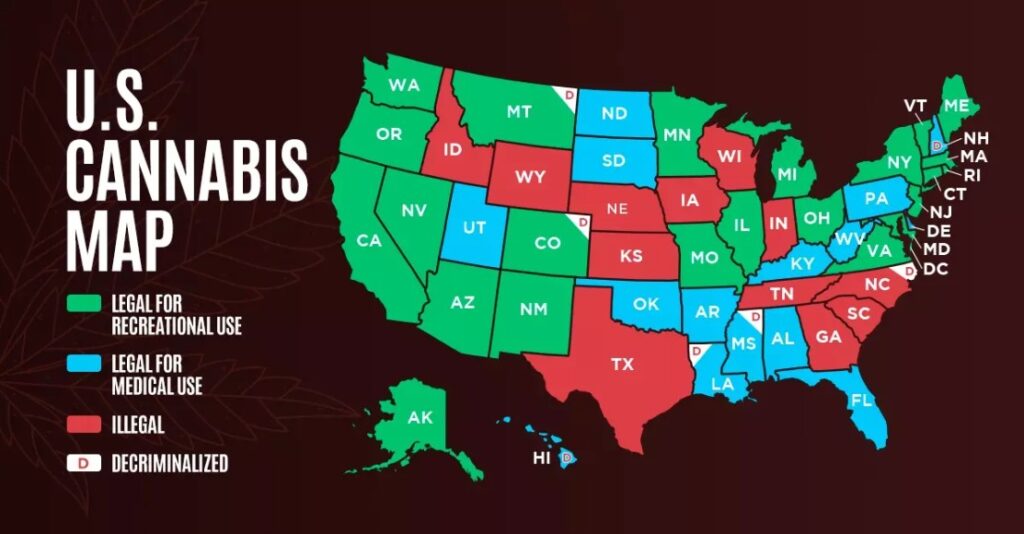
Image credit: [13]
One big question I have after looking at handfuls of journal articles on the subject is whether, in cases of negative brain impacts, those impacts are tied to the broad spectrum of cannabis compounds or if it just THC on its own. (Some studies cite general marijuana use; others specifically mention THC exposure in controlled lab studies.) Products at modern dispensaries are a far cry from what my parents smoked in the ‘60s, with isolated compounds and formulations designed for specific functions. If there is only a danger associated with THC, one could avoid (or at least limit) it with the right guidance (which can also be difficult to get from a dispensary employee who isn’t an expert in the subject).
Going back to last week’s post, [14] if CBD alone does not cause adverse effects on the brain (and has other health benefits), that seems like a clear win for CBD and Endocannabinoid System support. However, it’s not clear (to me, at least, at this point) if isolated CBD is free of adverse effects on the brain or if it works effectively without being paired with some THC – the jury appears to be out on that as well, again due to lack of available research in humans, [15] but there are indications that the body of scientific knowledge will continue to grow over the coming decade and more. Unfortunately, that doesn’t help those of us who want answers now, so (as is common in the field of public health), we’ll have to make informed decisions based on whatever information is available at the time and adjust our approach when new information becomes available.
~
This post was becoming too long to keep in one place, so now that we’ve covered some things we don’t know, we’ll be back next week with some things we do know (and what questions those have raised). Meanwhile, what questions do you have about anything here? And let me know if I got something wrong – I’m still learning.
Thanks for reading!
[1] https://radicalmoderate.online/stress-management-endocannabinoids/
[2] https://shop.mysterysupply.co/products/reefer-madness-1930s-exploitation-movie-poster
[3] https://www.scientificamerican.com/article/the-science-behind-the-dea-s-long-war-on-marijuana/
[4] https://www.healthline.com/health/narcotic-schedule
[9] https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2829657
[10] https://pmc.ncbi.nlm.nih.gov/articles/PMC5109019/
[11] https://www.medicalnewstoday.com/articles/does-weed-kill-brain-cells
[12] https://onlinelibrary.wiley.com/doi/abs/10.1111/add.13923
[13] https://covercannabis.com/blog/where-is-marijuana-legal/
[14] https://radicalmoderate.online/stress-management-endocannabinoids/
[15] https://premiumjane.com/blog/cbd-oil-without-thc/
1 Comment
Garrod · August 26, 2025 at 9:27 am
Another thought provoking blog…. I missed last week’s, so I’ll have to back and read it.
I always enjoy reading your blogs