Thank you for being here! Seven years ago this week, I was setting up this blog site and writing the very first post on recycling guidelines (for my neighbors, who didn’t know that there was a difference between what got collected for recycling and what actually got recycled). [1] The subsequent 365 weeks have involved explorations of all things sustainability, including topics of interest to me related to the environment, business, energy, cooking, travel, public health, and personal wellbeing. And, as is now tradition, I celebrate each year with a post related to the corresponding anniversary present. [2]
Since seven is the “Copper Anniversary,” I was tempted to look into the economically unsustainable production of the penny, [3] but I have a piece of copper hardware that has been far more integral to my life for most of the last decade: my IUD. For readers who are newer to this blog or haven’t seen any of my previous posts related to reproduction or menstruation, be warned that the contents of this post are not polite table conversation – and there will be personal anecdotes, descriptions of body parts, and photos. In short: abandon all squeamishness ye who enter here.
Options and Access
When last I checked, [4] 64.9% of the 72.2 million women aged 15-49 in the United States were using birth control (based on 2015-17 data). [5] That number has since dropped to 54.3% in the 2022-23 data. [6] My jaw dropped too when I saw those numbers, but a lot of things have changed in the days since the Dobbs decision. I have heard anecdotally that there has been more general confusion about what contraceptives are currently legal (or on the political chopping block), but we can observe statistical changes in behavior from before and after Roe v. Wade was overturned. For example, one study found “statistically significant evidence that sexual activity declined, barriers to accessing contraception increased, [and] reports of receiving high-quality contraceptive care decreased.” [7]
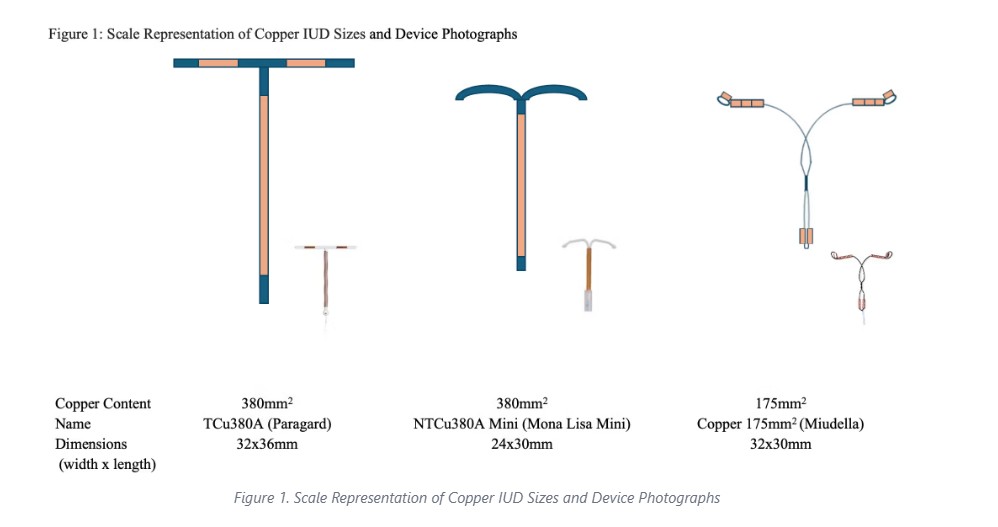
Image credit: [8]
In both reports referenced above, long-acting reversible contraceptives (which include intrauterine devices) were the third-most common option in use, after female sterilization (18.6% → 11.5%) and the oral contraceptive pill (12.6% → 11.4%), and ahead of the male condom (8.7% → 7.1%). It was also the only option to stay relatively stable in percentage in the reports between those years, and even increased ever so slightly (10.3% → 10.5%). The fact is that in many cases, the IUD does make for a relatively convenient and effective method of contraception that is minimally invasive and doesn’t require a change in behavior. When I got my first one in 2017, I was told that it was 99% effective, which are about as good odds as you’re going to get with contraceptives. I went to Planned Parenthood for my appointment because I didn’t have great health insurance, and they were affordable. (They now get my gratitude as well as the largest of all my automated monthly donations.)
The biggest decision I had to make at the time was whether I wanted a hormonal or non-hormonal IUD. The non-hormonal IUD makes use of exposed copper coils to make the uterus an inhospitable environment for sperm. The primary function of the copper is to kill sperm and prevent them from fertilizing the egg. The hormonal IUD thickens the layer of cervical mucus, preventing sperm from reaching the egg; it also thins the layer of uterine lining, preventing a fertilized egg from implanting. [9] The fact that these devices could prevent implantation of a fertilized egg (even though that is not the primary function of the copper IUD), is why IUDs are high on the list of at-risk contraceptives in many states. [10]
Safety and Effectiveness
I ultimately opted for the copper IUD (ParaGard) because I was pretty fed up with hormonal birth control wreaking havoc on my mood and my weight for the previous ten years. The downside of the copper IUD is “heavier periods and cramping,” which I would say was a bit of an understatement. In fact, many people change their mind about IUDs after they’re inserted because of continued intense discomfort and bleeding. (Also, in some cases, their bodies simply expel the foreign object.) As it happens, I had my first one for less than two years (after accidentally pulling it out of position with my menstrual cup, [11] making it both painful and ineffective). Right around the time I was figuring out what to do next, a friend told me about a clinical study for a new type of IUD.

According to the Food and Drug Administration, IUDs are considered a device/drug combination, which means they require extensive clinical trials before approval. One such clinical trial was getting started just when I needed a new IUD. The study would give 20% of participants the ParaGard (TCu380A) and 80% of participants the Mona Lisa (NT Cu380-Mini), a smaller device already approved in Europe and Canada, which was intended to result in less insertion pain, as well as lighter cramping and bleeding, than the ParaGard. It was a single-blind study, so I wouldn’t know which one I got until the end of the 3-year study when it had to come back out. And since insertion pain was one of the data points tracked in the study, I was not allowed any numbing agents. (Shaking my fist at men who get general anesthesia for vasectomies…) Although I was pretty sure I got the Mona Lisa, it wasn’t exactly a walk in the park.
The study involved completing daily worksheets to track pain, bleeding, and sexual activity over the first year, as well as attending checkups every few months, first in person and later by phone. I actually enjoyed the novelty of it all (and I got paid for participating, which wasn’t bad either.) Mostly, I was excited to be taking part in something that could broaden contraceptive options for women in the United States. At my last appointment, right before the IUD came out, the doctor asked which one I thought I had. With amusement, I realized that this moment would likely be the only such “let’s see what we’ve got here” situation I’d ever experience, since I wouldn’t be having children.
Mona Lisa and Miudella
I got another ParaGard again after the study, and my husband got a vasectomy the following year, so contraception really has not recently been on my mind until I thought to write about it for my Copper Anniversary post. (Again, I recognize how privileged I am not to have to worry about that now. It absolutely consumed my thoughts during the 10 months between the Dobbs decision leak and Christian’s surgery, even though I had an IUD at the time.) As it happens, the Mona Lisa study ended in 2022, and it still hasn’t been approved by the FDA. I looked into the situation for this post and got a kick out of reading the study on PubMed, knowing that I was one of the 732 “nulliparous women” who received the test IUD. [12]
It wasn’t surprising to see that the Mona Lisa had lower discontinuation rates due to pain and bleeding, or that it had lower expulsion rates, compared to the control IUD. What was surprising was that the “NTCu380 Mini [Mona Lisa] had a 3-year cumulative pregnancy rate of 4.8% compared to 2.5% for the TCu380A [ParaGard].” I read that statistic to Christian while writing this post, and we both stared at each other quietly as though we’d dodged a bullet. I also wasn’t thrilled to hear that the pregnancy rate with ParaGard rate was 2.5% when it was always my understanding that it was less than 1%. As it happens, more modern studies put ParaGard pregnancy rates at around 3%, 1-2% higher than hormonal IUDs. [13] Once again, I am grateful that my husband is among the small but growing percentage of US men who have opted for a vasectomy. (Numbers were already on the rise from 2014, but insurance data indicated another bump after Dobbs. [14])
While Mona Lisa hasn’t yet met with FDA approval (and likely won’t, thanks to the high pregnancy rate), another model, Miudella (study name “Veracept”) was approved by the FDA in February 2025 (the first non-hormonal IUD to be approved by the FDA in over 40 years) and is apparently coming to market in early 2026. Like the Mona Lisa, it is smaller than the ParaGard, but it is made of nickel-titanium alloy with copper beads on the arms. It is flexible, which studies indicate may be a bigger factor than size when it comes to reducing pain. It is approved for 3 years, and it has a 3-year cumulative pregnancy rate of 1.26%. Because it is a slightly different shape and has a slightly different insertion process, it can only be sold to certified providers, meaning clinicians will need to go through a training and certification process. [15] This extra step is intended to ensure patient safety and product efficacy, but some are concerned that it might make the device less accessible in an environment where access to quality reproductive healthcare is already limited.
~
I don’t need to go into a rant here about the benefits of bodily autonomy for women (i.e. better health and safety outcomes, higher levels of education and income, etc.) – I’ve done that before, and it’s worth a read. [16] But I do worry about freedom of choice and access to quality healthcare, especially now when those things are under attack. The posts I’ve written over the last seven years don’t always end on an upbeat note – like this one, some are a reminder that we have to create the world we want to see. For me, that means voting for my priorities in every election, telling my elected officials how I feel between elections, and supporting groups that are doing valuable work to fill the growing gaps in our social safety net.
There’s so much more I wanted to write about in this post, but it will have to wait for another time. For now, I’d be curious (to the extent you’re comfortable sharing) about your own experiences, questions, and thoughts on the subject.
Thanks for reading!
[1] https://radicalmoderate.online/new-recycling-guidelines-in-the-south-hills/
[2] https://radicalmoderate.online/tag/anniversary/
[4] https://radicalmoderate.online/vasectomies/
[5] https://www.cdc.gov/nchs/products/databriefs/db327.htm
[6] https://www.cdc.gov/nchs/products/databriefs/db539.htm
[7] https://academic.oup.com/healthaffairsscholar/article/2/2/qxae016/7603817?login=false
[8] https://www.contemporaryobgyn.net/view/contraception-year-in-review-2025
[9] https://whsobgyn.com/copper-vs-hormonal-iuds/
[10] https://stateline.org/2022/05/19/some-states-already-are-targeting-birth-control/
[11] https://shopdiva.com/collections/diva-cup-series
[12] https://pmc.ncbi.nlm.nih.gov/articles/PMC9294241/
[13] https://www.contemporaryobgyn.net/view/contraception-year-in-review-2025
[14] https://www.uchicagomedicine.org/forefront/surgery-articles/vasectomy-trends-research
[15] https://www.contemporaryobgyn.net/view/contraception-year-in-review-2025
0 Comments